The Simple Medical Diagnostics That Are Changing Healthcare
For developing countries, diagnostics can be expensive and impractical. A group of scientists is hoping to change that.
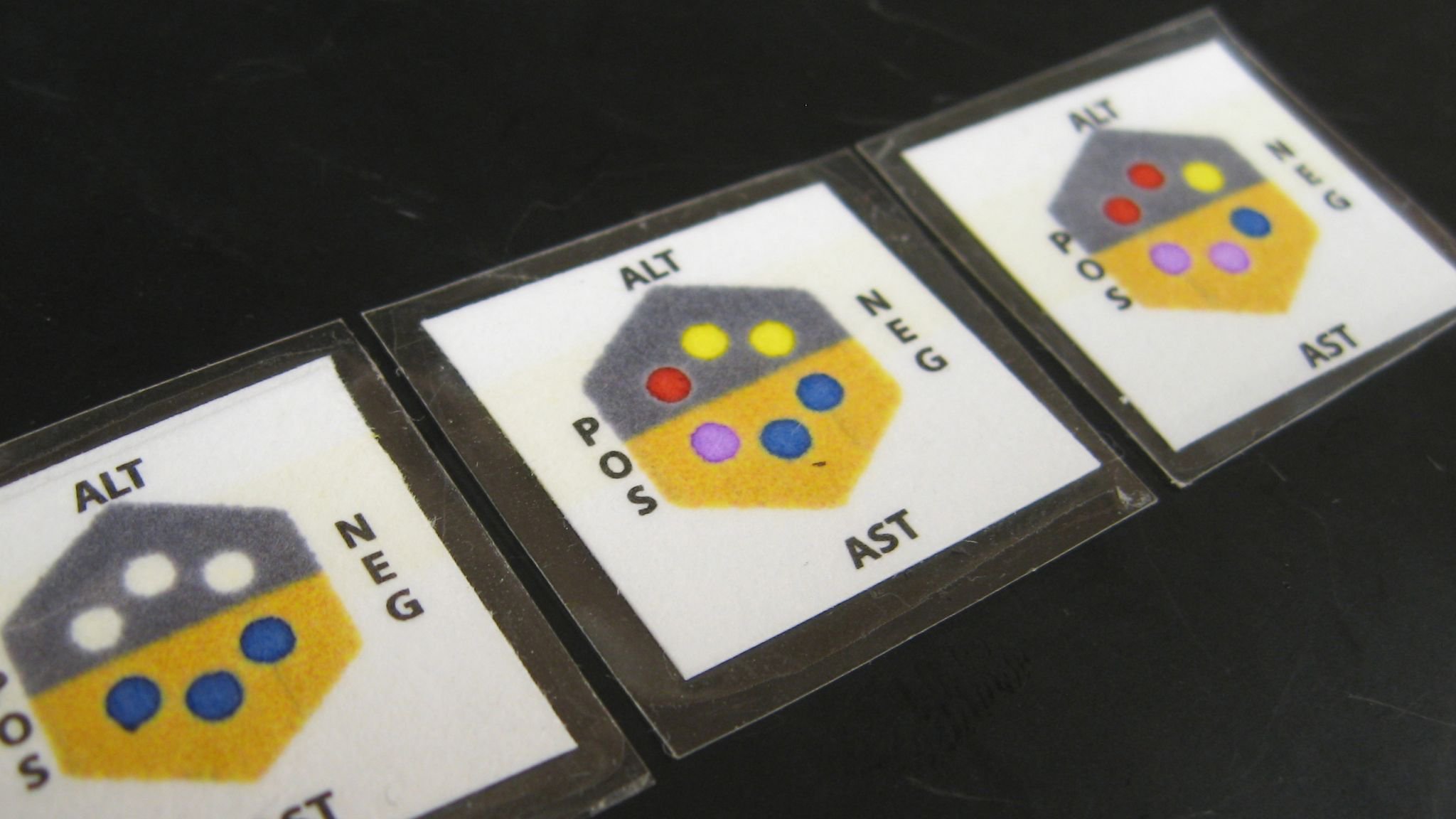
George Whitesides's lab originally developed the paper-based technology behind this liver function test from the nonprofit Diagnostics for All. Image Credit: Diagnostics for All
As a child in Nigeria, Onyx Adegbola contracted malaria. She would come down with the typical symptoms—fever and body aches, nausea, and headaches—and to ease her suffering, she would take anti-malarial tablets. But here’s the thing. One isn’t supposed to self-diagnose malaria; there are simple tests you can perform instead to confirm it is malaria and not some other disease. The definitive one involves examining a blood smear under a microscope, but microscopes were—and are—relatively scarce in that part of the world. So are clinical laboratories.
Related

The Quest for a Simple Cancer Test

Could a Smartphone App Diagnose Your UTI Faster than the Lab?

Malaria is outsmarting blood tests. Can a breath test help?
So Adegbola took the tablets and hoped for the best. Fortunately the pills worked. But not everyone is so lucky. “One of my sister’s friends died at the age of 18 because she had a fever and they thought it was malaria, but it was typhoid fever,” she says. “It was eminently treatable…but she died because there was no diagnosis.”
“If you could spend another $100 per person on healthcare in developing countries, the outcomes you could make would be incredible.”
Today, Adegbola, an MD PhD who has worked in the pharmaceutical, medical device, and diagnostics industries, is hoping to rewrite such stories through a “very early stage” venture she co-founded called A’as Inc. A’as is one of a small but growing number of companies looking to bring cutting-edge clinical diagnostics technologies from Western bench tops to the developing world, where it’s difficult to understate their life-saving potential. “Say you spend another $100 a year per person in the United States. The outcomes you get don’t make a lot of difference,” says David Erickson, a professor and diagnostics developer at Cornell University. “But if you could spend another $100 per person in a lot of other places, the outcomes you could make would be incredible.”
It won’t be easy to get there—infrastructure, money, and other hurdles stand in the way. But researchers are determined to try. Indeed, those struggles are implied in Adegbola’s company’s name. A’as is “the Hittite god of wisdom,” she explains. “We’re going to need a lot of wisdom in this venture.”
Building Tools for the Developing World
When it comes to migrating medical technology to “resource-poor” environments like Africa, Latin America, and Southeast Asia, you can take nothing for granted. Electricity, clean running water, supply chains, and refrigeration may all be unreliable. Medical personnel may be untrained, and even if they’re not, may lack the equipment to run tests taken for granted in developed countries, or the parts to repair it when it breaks.
Patient interactions, too, are different than in the developed world, says George Whitesides, a professor of chemistry at Harvard University. The doctor’s office isn’t always a short bus-ride away—in some places, it may be a two-day walk. That means there are rarely opportunities for a follow-up visit, so diagnostics and treatment decisions need to be turned around quickly. “Whatever you’re going to do with them, either it has to be done then and there or not at all.”
And then, of course, there’s the economics. American and European pricing is obviously unrealistic in such areas. But even tests costing just a dollar apiece can stumble. Amit Agarwal, principal for life sciences at Deloitte Consulting in San Francisco, recalls a client that was looking to deploy a certain diabetes test in India, a potentially huge market. Most American diabetics monitor their disease using a glucometer, which measures blood sugar. In India, diabetics frequently use a far less expensive, but also less accurate, urine strip. But even then, the test was too expensive, Agarwal says: Users would “cut it in half very carefully so they could actually get more than a single test out of it.”
That anecdote shows that successful tests need to be at least “an order of magnitude less” expensive than Western markets to succeed in the developing world, Agarwal says. But cost alone doesn’t spell success; developers must also figure out how to ensure everyone in the supply chain can make money or the product will never get out to where it’s needed.
Some companies are particularly savvy in this regard, he says, taking their cues from consumer product manufacturers. Throughout India, for instance, street vendors sell a kind of betel nut chewing gum called paan . These vendors add various toppings, including tobacco. Tobacco distributors obviously understand how the distribution system works, and so to distribute its diabetes test, Agarwal says his client partnered with one. Success, he says, “takes the mentality of … a Coca-Cola marketer for Africa tied together with somebody that’s an absolutely altruistic, wants-to-save-the-world kind of person to develop the technology.”
PCR Powered by the Sun
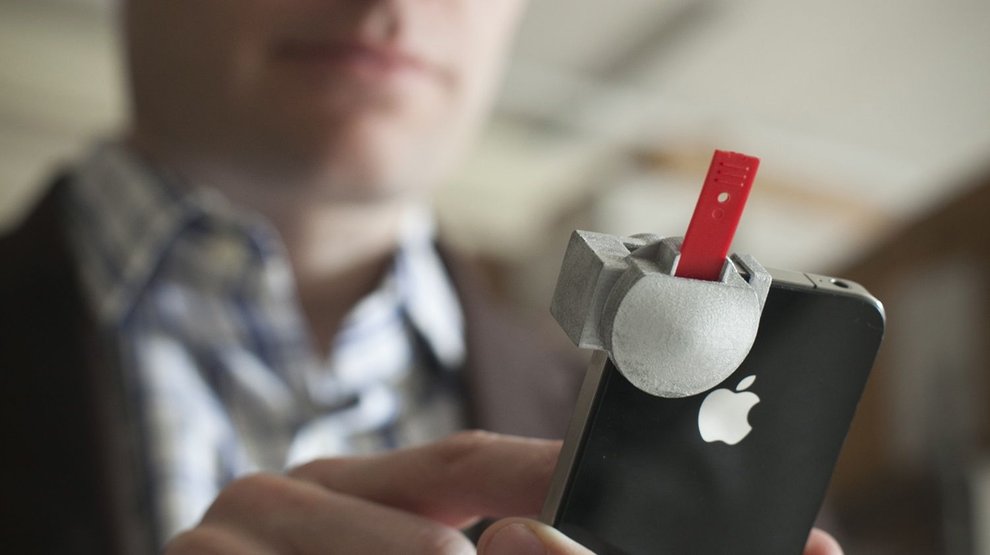
At Cornell University in New York, David Erickson’s lab develops low-cost diagnostics that piggyback on smartphones, which are essentially powerful battery-operated computers preconfigured with geolocation, communications, and imaging. They are inexpensive, broadly available, and easy to use, making for an ideal diagnostics platform, he explains.
Erickson’s lab focuses on nutrition-based diagnostics that work something like a pregnancy test. His vitamin D test comprises a small rectangular device that sits over the phone’s camera and a test strip that plugs into the device. That strip runs an immunoassay, an antibody-based test that changes the strip’s color based on vitamin concentration. The phone’s camera records that color change, and a custom app converts it into a number that people can use to test whether or not a patient is malnourished. He calls the device a “Nutriphone.” “Knowledge of these [nutrition] markers allows people to make changes to their diets that may improve their nutritional status.”
More recently, Erickson has turned his attention to infectious diseases. His team developed a PCR machine—a device used to diagnose diseases by quantifying nucleic acids like DNA or RNA—that runs on the sun. PCR machines typically use electricity to cycle the heating and cooling phases of a multistage, carefully timed reaction that occurs in tubes placed a metal block. The heart of Erickson’s device are the meandering channels of a microfluidic disk, which consists of miniaturized circuits through which fluids flow at controlled rates. As they move through the disk, the fluids pass back and forth through three distinct temperature zones. Those zones are created using photomasks that allow more or less sunlight to hit the disk, and the timing is governed by the length of the channels. An attached smartphone records the reaction temperatures to ensure the device ran as intended and reads the result, again using the camera.
Erickson’s team used that platform to build an assay for Kaposi’s sarcoma, a cancer common in AIDS patients, and traveled to Uganda and Kenya to test it. Aggrey Semeere, a physician at the Infectious Diseases Institute in Kampala, Uganda, worked with Erickson on those early tests, in which five samples were prepared and run.
One of the key benefits of such a point-of-care device, Semeere says, is that it can lessen the time between diagnosis and treatment. At the moment, patients typically not only travel from rural health center to larger urban centers to regional centers, but then they have to look for someone with the skills and time to collect and interpret a biopsy. “Usually they give up before they even make it to the top,” he says, and those who do make it must wait a long time for their results. All the while the disease is progressing without a formal diagnosis being made.

Erickson’s solar PCR system, which is to be commercialized by A’as, should streamline the process. “It just needs a basic lab running with a lab technician who you can teach how to run the machine or …understand how it works,” Semeere says. “And that gap and that time will be [reduced].”
The device got off to a rocky start, however. According to Semeere, Erickson had previously tested the device on fresh-frozen specimens, but in Uganda most biopsies are chemically fixed in formaldehyde, and the system struggled with those samples. “There’s some changes in the DNA that happen when you throw the samples in that chemical,” he says. More to the point for a solar-powered device, it was cloudy during Erickson’s brief stay, and the team had to test their device using a solar lamp powered by a cell phone battery. Still, says Semeere, the team considered the trip successful. “It’s at a point where we are ready to roll out a wider pilot.”
Microfluidic Devices Made From Paper
Whitesides says, fundamentally, there are two approaches that researchers can take to adapt Western diagnostics to the developing world. They can, as Erickson did, take an existing technique and try to make it simpler, lower power, and less expensive. Or, they can try to redesign the system from the bottom up with those goals in mind from the start. “The latter point of view has the interesting characteristic that as you start developing these low-cost methods, what you find is there are things you can do with low-cost technology that you can never do with high-cost technology,” Whitesides explains.
Whitesides, for instance, has for many years been studying the properties and applications of microfluidic devices made of a soft rubbery material called PDMS. But for diagnostics work, he opted instead to build devices out of paper—a transition that makes them lighter, cheaper, and easier to use and produce. “If you want to build three-dimensional microfluidic systems in PDMS, you can do it, but it’s a real nuisance. It’s absolutely straightforward in paper. Just essentially trivial.”
His lab has developed paper-based enzyme assays for applications like liver function, which must be monitored in patients on certain antiviral and anti-tuberculosis treatment regimens. Built of two strips of paper and a membrane sandwiched between laminated sheets, the device takes a droplet of blood, separates the plasma from the cells, and then incubates that plasma with chemicals that report the activity of two key liver enzymes, alanine aminotransferase and aspartate aminotransferase. The result is a color change in a detection window that correlates with liver damage.
A Boston-based nonprofit called Diagnostics for All (DFA) has been developing that diagnostic, and has published a field trial on 600 individuals in Vietnam. The company also is developing tests for such applications as immunity assessment (to monitor vaccinations) and animal husbandry (detecting cow estrus).
More recently, Whitesides’ team has turned its attention to glucometers. Glucometers, Whitesides explains, are widely available and inexpensive, but perform only a single task and are built on outdated technology. Alex Nemiroski, a postdoctoral fellow in the lab, reengineered the device to produce a flexible testing platform in approximately the same form factor from modern off-the-shelf components, including a powerful Arduino microprocessor, a multipurpose computer beloved by DIY computer enthusiasts.
The resulting system, Whitesides says, “will do literally any electrochemical assay you can think of,” selected simply by pressing a button on the device’s face. His team has used the system to quantify glucose in blood, lead in water, sodium in urine, and a malarial antigen in buffer, sending results to a remote computer—at a central hospital, say—via text message from an inexpensive cell phone. Seconds later, the computer acknowledges receipt and provides an interpretation.
The multipurpose system has quantified glucose in blood, lead in water, sodium in urine, and a malarial antigen in buffer.
One key benefit of such a system is public health monitoring, Whitesides says. Take Dengue fever, for instance. There is no treatment for that disease, he notes. But, if enough people come down with the disease—something that such a device theoretically could monitor—public health officials could then spray for mosquitoes.
Indeed, when it comes to diagnostics for the developing world, says Matthew Hudes, Deloitte’s managing principal for biotechnology in the U.S., the key word is “actionable.” “Is there some action that you can take, as a medical professional, to make a difference?” Such devices tend to focus less on the cutting edge of what technology can do, but rather what is reasonable and can impact healthcare and treatment. Erickson, for instance, focuses on markers of nutrition, which he calls “the world’s biggest problem,” and Whitesides on diagnostics.
“All the assumptions have to be different” in the developing world, Whitesides says. “And it really makes you think less along the idea of fancy widgets, and more along the idea of how do you get technology that really works practically for a reasonable number of people and for the public health system at low cost and great simplicity.”
Not Just for the Third World
That’s not to say such devices don’t have value in the U.S. and other Western markets, however. Indeed, sales in developed regions could help finance a company’s less lucrative efforts, Agarwal says. He cites, for instance, GE’s handheld Vscan ultrasound. Conceived and manufactured in Asia for use by hospitals that cannot afford conventional ultrasound machines, the Vscan now is gaining market share in the U.S., where it is used for rapid testing in the ER.
Similarly, it’s easy to imagine handheld point-of-care devices for flu, antibiotic resistance, blood chemistry, and more—tools that could have a place in a doctor’s office or ambulance rather than just the laboratory. Marcus Lovell Smith, CEO of DFA, suggests an application to facilitate routine patient monitoring in clinical trials. Patients disinclined to come to a clinic for routine blood work could test themselves at home, thereby enhancing patient retention and saving companies money. “Retaining patients in the trial, given the cost of recruitment, is very important,” he says, “so having tools that make life easier for those patients while you’re still obtaining the information you want could be useful.”
But it is in resource-poor places like Africa where such tools likely will have the biggest impact. Growing up in Lagos, Adegbola had no idea how bad things were in Nigeria’s rural villages until she visited as a medical student. “It’s a completely different mindset, a completely different set of problems. The impact that this could have is just staggering.”
Photo credits: Diagnostics for All and David Erickson
 Jeffrey PerkelPosts By This Contributor
Jeffrey PerkelPosts By This Contributor